
In the context of personalized medicine, this design is used when the biomarkers are only putative or not known at the beginning of a Phase II trial and is also useful when there are multiple targeted treatments and biomarkers to be considered. It aims to test simultaneously both biomarkers and treatments while providing more patients with effective therapies according to their biomarker profiles. Outcome-adaptive randomization is sometimes included under the umbrella of “Bayesian clinical trials” but as criticized by Korn and Freidlin (2011), there is nothing inherently Bayesian about it.
Alternative names: Adaptive randomization, Bayesian Adaptive, Bayesian Adaptive randomization, Combined dynamic multi-arm, Outcome-Adaptive randomization, Outcome-based Bayesian Adaptive Randomization
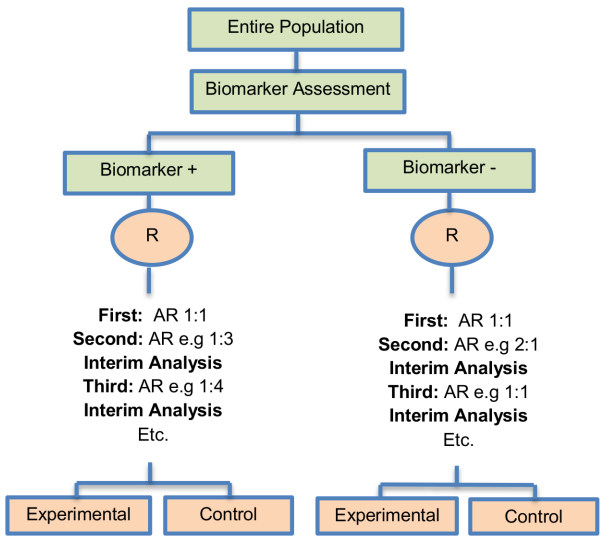
Adaptations: Change in randomization ratio
Details
Methodology
- The process starts with the biomarker profile assessment of all eligible patients and then according to the profile of each individual, the study population will be assigned to the different biomarker groups. Due to the fact that at the beginning of the trial we do not know the true disease control rate (i.e., the proportion of patients who demonstrate response to a treatment) the trial begins with equal randomization so that each treatment by biomarker subgroup is composed of at least one individual with a known disease control status (whether the patient will experience progression given a certain treatment).
- Next, the trial continues with adaptive randomization of patients; this is achieved by using the Bayesian probit model to calculate the posterior disease control rate. After the posterior rate is found, we define the randomization rate as the posterior mean of the disease control rate of each treatment in each biomarker-defined subgroup.
- The adaptive randomization process continuous until the last individual is enrolled and can stop early only in case that all treatments are dropped due to inefficacy.
Note: Whereas in many trial designs the baseline covariate (in this case the biomarker) is considered as prognostic, the design proposed by Zhou et al. (2008) allows for modelling the treatment by biomarker interactions where the biomarker is in fact predictive. The incorporation of the above hierarchical Bayesian structure allows ‘borrowing strength’ or information-sharing across patients receiving the same treatment but with different biomarker profiles, Zhou et al. (2008).
Statistical/Practical considerations
Advantages
- Smart, novel and ethical approach
- Permits updating patient's outcome.
- Can result in high probability of success of the trial as there is increase in the number of patients who receive effective treatments.
- Type I and II errors can be controlled by carefully calibrating the design parameters
- Can boost patients' ethics as patients are assigned to the best available therapy
Limitations
- Complexity in terms of building-up the trial design, conduct and analysis of the trial
- Can make incorrect decisions in case of incorrect biomarker selection as the design is based on the accumulated data about how well the biomarker performs.
- Requirement of relatively short biomarker and endpoint assessment
- Likely to introduce bias due to time trends in the prognostic mix of individuals enrolled to the study.
Key references
-
Gosho M, Nagashima K, Sato Y. Study designs and statistical analyses for biomarker research. Sensors (Basel, Switzerland). 2012;12(7):8966–86. doi: 10.3390/s120708966. View Article PubMed/NCBI Google Scholar
-
Lee JJ, Xuemin G, Suyu L. Bayesian adaptive randomization designs for targeted agent development. Clinical trials (London, England). 2010;7(5):584–96. doi: 10.1177/1740774510373120. View Article PubMed/NCBI Google Scholar
-
Mandrekar SJ, Sargent DJ. Clinical trial designs for predictive biomarker validation: theoretical considerations and practical challenges. Journal of clinical oncology: official journalof the American Society of Clinical Oncology. 2009;27(24):4027–34. doi: 10.1200/JCO.2009.22.3701. View Article PubMed/NCBI Google Scholar
-
Kelloff GJ, Sigman CC. Cancer biomarkers: selecting the right drug for the right patient. Nature reviews Drug discovery. 2012;11(3):201–14. doi: 10.1038/nrd3651. pmid:22322254 View Article PubMed/NCBI Google Scholar
-
Chow S-C, Tu Y-H. On Two-stage Seamless Adaptive Design in Clinical Trials. Journal of the Formosan Medical Association = Taiwan yi zhi. 2008;107(12 Suppl):52–60. pmid:19129046 View Article PubMed/NCBI Google Scholar
-
Chow S-C, Chang M. Adaptive design methods in clinical trials—a review. Orphanet journal of rare diseases. 2008;3:11-. doi: 10.1186/1750-1172-3-11. pmid:18454853 View Article PubMed/NCBI Google Scholar
-
Freidlin B, Korn EL. Biomarker-adaptive clinical trial designs. Pharmacogenomics. 2010;11(12):1679–82. doi: 10.2217/pgs.10.153. pmid:21142910 View Article PubMed/NCBI Google Scholar
-
Galanis E, Wu W, Sarkaria J, Chang SM, Colman H, Sargent D, et al. Incorporation of biomarker assessment in novel clinical trial designs: personalizing brain tumor treatments. Current oncology reports. 2011;13(1):42–9. doi: 10.1007/s11912-010-0144-x. pmid:21125354 View Article PubMed/NCBI Google Scholar
-
Ang M-K, Tan S-B, Lim W-T. Phase II clinical trials in oncology: are we hitting the target? Expert review of anticancer therapy. 2010;10(3):427–38. doi: 10.1586/era.09.178. pmid:20214523 View Article PubMed/NCBI Google Scholar
-
Berry DA. Bayesian clinical trials. Nature reviews Drug discovery. 2006;5(1):27–36. doi: 10.1038/nrd1927. pmid:16485344 View Article PubMed/NCBI Google Scholar
-
Scher HI, Nasso SF, Rubin EH, Simon R. Adaptive clinical trial designs for simultaneous testing of matched diagnostics and therapeutics. Clinical cancer research: an official journal of the American Association for Cancer Research. 2011;17(21):6634–40. doi: 10.1158/1078-0432.CCR-11-1105. View Article PubMed/NCBI Google Scholar
-
Berry DA, Herbst RS, Rubin EH. Reports from the 2010 Clinical and Translational Cancer Research Think Tank meeting: design strategies for personalized therapy trials. Clinical cancer research: an official journal of the American Association for Cancer Research. 2012;18(3):638–44. doi: 10.1158/1078-0432.CCR-11-2018. View Article PubMed/NCBI Google Scholar
-
Tajik P, Zwinderman AH, Mol BW, Bossuyt PM. Trial designs for personalizing cancer care: a systematic review and classification. Clinical cancer research: an official journal of the American Association for Cancer Research. 2013;19(17):4578–88. doi: 10.1158/1078-0432.CCR-12-3722. View Article PubMed/NCBI Google Scholar
-
Di Maio M, Gallo C, De Maio E, Morabito A, Piccirillo MC, Gridelli C, et al. Methodological aspects of lung cancer clinical trials in the era of targeted agents. Lung cancer (Amsterdam, Netherlands). 2010;67(2):127–35. doi: 10.1016/j.lungcan.2009.10.001. View Article PubMed/NCBI Google Scholar
-
Wason JMS, Trippa L. A comparison of Bayesian adaptive randomization and multi-stage designs for multi-arm clinical trials. Statistics in medicine. 2014;33(13):2206–21. doi: 10.1002/sim.6086. pmid:24421053 View Article PubMed/NCBI Google Scholar
-
Sato Y, Laird NM, Yoshida T. Biostatistic tools in pharmacogenomics—advances, challenges, potential. Current pharmaceutical design. 2010;16(20):2232–40. pmid:20459388 View Article PubMed/NCBI Google Scholar
-
Korn EL, Freidlin B. Outcome—adaptive randomization: is it useful? Journal of clinical oncology: official journal of the American Society of Clinical Oncology. 2011;29(6):771–6. doi: 10.1200/JCO.2010.31.1423. View Article PubMed/NCBI Google Scholar
-
Lai TL, Lavori PW, Shih M-CI, Sikic BI. Clinical trial designs for testing biomarker-based personalized therapies. Clinical trials (London, England). 2012;9(2):141–54. doi: 10.1177/1740774512437252. View Article PubMed/NCBI Google Scholar
-
Gold KA, Kim ES, Lee JJ, Wistuba II, Farhangfar CJ, Hong WK. The BATTLE to personalize lung cancer prevention through reverse migration. Cancer prevention research (Philadelphia, Pa). 2011;4(7):962–72. doi: 10.1158/1940-6207.CAPR-11-0232. View Article PubMed/NCBI Google Scholar
-
Lai TL, Liao OY-W, Kim DW. Group sequential designs for developing and testing biomarker-guided personalized therapies in comparative effectiveness research. Contemporary clinical trials. 2013;36(2):651–63. doi: 10.1016/j.cct.2013.08.007. pmid:23994669 View Article PubMed/NCBI Google Scholar
-
Younes A, Berry DA. From drug discovery to biomarker-driven clinical trials in lymphoma. Nature reviews Clinical oncology. 2012;9(11):643–53. doi: 10.1038/nrclinonc.2012.156. pmid:22965151 View Article PubMed/NCB Google Scholar
-
Buyse M, Michiels S, Sargent DJ, Grothey A, Matheson A, de Gramont A. Integrating biomarkers in clinical trials. Expert review of molecular diagnostics. 2011;11(2):171–82. doi: 10.1586/erm.10.120. pmid:21405968 View Article PubMed/NCBI Google Scholar
-
Zhou X, Liu S, Kim ES, Herbst RS, Lee JJ. Bayesian adaptive design for targeted therapy development in lung cancer—a step toward personalized medicine. Clinical trials (London, England). 2008;5(3):181–93. doi: 10.1177/1740774508091815. View Article PubMed/NCBI Google Scholar
-
European Medicines Agency. Reflection paper on methodological issues associated with pharmacogenomic biomarkers in relation to clinical development and patient selection London; 2011 [updated [cited 2012 Jul 3]; cited 2015 10 Oct]. Available from: http://www.ema.europa.eu/docs/en_GB/document_library/Scientific_guideline/2011/07/WC500108672.pdf .
-
Liu A, Liu C, Li Q, Yu KF, Yuan VW. A threshold sample-enrichment approach in a clinical trial with heterogeneous subpopulations. Clinical trials (London, England). 2010;7(5):537–45. doi: 10.1177/1740774510378695. View Article PubMed/NCBI Google Scholar
Variations:
Bayesian covariate adjusted response-adaptive randomization
-
Description: The Bayesian Covariate Adjusted Response-Adaptive Randomization (BCARA) which combines a Bayesian, an adaptive and biomarker classification approach aims to match patients with the most efficacious treatments by utilizing patient’s biomarker information becoming available during the conduct of the clinical trial. It is also considered as a response-adaptive randomization strategy as the allocation of the study population depends on the responses of previous outcomes. A partial least square logistic regression approach is conducted to determine adaptively predictive biomarker-defined subsets.
-
Application: This strategy may be useful in the explanatory phase II setting of the drug development .
- Alternative names: No alternative names found for this trial deisgn
-
Methodology:
1. R andomly assign the first
 patients
to the different treatment arms where J the
number of different treatment groups and K
the number of biomarkers. At least one
response should be observed in each of the
different treatment groups before moving to
the Bayesian response adaptive randomization
patients
to the different treatment arms where J the
number of different treatment groups and K
the number of biomarkers. At least one
response should be observed in each of the
different treatment groups before moving to
the Bayesian response adaptive randomization
2. A fter each new individual has been enrolled in the study, predictive biomarker-defined groups are determined by utilizing a partial least squares logistic regression strategy (PLSLR) which can predict whether the patient can benefit from the treatment. The biomarker status is determined before the randomization .
3. A fter the establishment of the biomarker status and biomarker-defined groups of each new individual, the individual is then randomly assigned into one of the treatment arms using a BCARA randomization .
4. A ccording to the results of the BCARA randomization the trial either stops or continues based on decision rules proposed by Eickhoff et al. (2010) [53]. The Bayesian covariate adjusted response-adaptive trial design has the ability to identify the biomarker-defined groups likely to respond to a treatment but it does not control the Type I error and in order to ensure that the identified result is true, a Phase III study should be conducted
- Adavantages and limitations:
| Advantages | Limitations |
|
Ability to incorporate prior knowledge from biomarkers into the design.
Identification of the
subgroups for which a particular
experimental treatment is more
effective. Can result in reduction of the number of patients required when compared to alternative designs (i.e, non-adaptive trial designs). Solves the issue of the incorporation of information of multiple and possibly correlated biomarkers. |
The Type I error is not controlled in the traditional sense. An independent Phase III study focused on the selected biomarker-defined subgroups is required to show that the identified promising result is definitely true.
|
- References:
Eickhoff JC, Kim K, Beach J, Kolesar JM, Gee JR. A Bayesian adaptive design with biomarkers for targeted therapies. Clinical trials (London, England). 2010;7(5):546–56. doi: 10.1177/1740774510372657. View Article PubMed/NCBI Google Scholar
Tajik P, Zwinderman AH, Mol BW, Bossuyt PM. Trial designs for personalizing cancer care: a systematic review and classification. Clinical cancer research: an official journal of the American Association for Cancer Research. 2013;19(17):4578–88. doi: 10.1158/1078-0432.CCR-12-3722. View Article PubMed/NCBI Google Scholar
